Most men will spend more time researching a car purchase than they will asking a doctor about a concern that has been quietly affecting their confidence, their sleep, and their relationships for months. Not because they don’t care — but because no one ever gave them a clear, judgment-free place to start.
This is that place.
What follows is a complete, medically grounded guide to men’s sexual health: what it actually means, what changes are normal across different decades of life, which symptoms deserve professional attention, and what you can do — starting today — to protect your long-term well-being. No unnecessary alarm. No vague reassurances. Just the information you actually need.
Key Takeaways
- Men’s sexual health involves physical, hormonal, mental, and relational dimensions — not just the absence of disease or dysfunction.
- Testosterone levels decline gradually after age 30 at approximately 1–2% per year, but a significant drop is a diagnosable, treatable condition — not an inevitable consequence of aging.
- Erectile difficulties in men under 50 are sometimes the earliest clinical indicator of underlying cardiovascular issues.
- An estimated 20–30% of men experience premature ejaculation at some point — it is the most common male sexual dysfunction, and it responds well to evidence-based interventions.
- Many STIs produce no symptoms in men. Routine testing is the only reliable method of knowing your status.
What Men’s Sexual Health Actually Means
Sexual health is not simply the absence of dysfunction. The World Health Organization defines it as a state of physical, emotional, mental, and social well-being in relation to sexuality — not merely the absence of illness or impairment.
For men specifically, this means being able to engage in sexual activity comfortably when desired, understanding how your body functions across different life stages, being free from sexually transmitted infections or managing them appropriately if present, and feeling equipped to communicate openly with partners about health, needs, and boundaries.
Men’s sexual health is not a fixed state. It shifts with age, stress levels, relationship quality, physical health, and lifestyle choices. That variability is not a flaw — it is a normal feature of a living system. Understanding it is the foundation of taking care of yourself well.
The Four Dimensions of Men’s Sexual Health
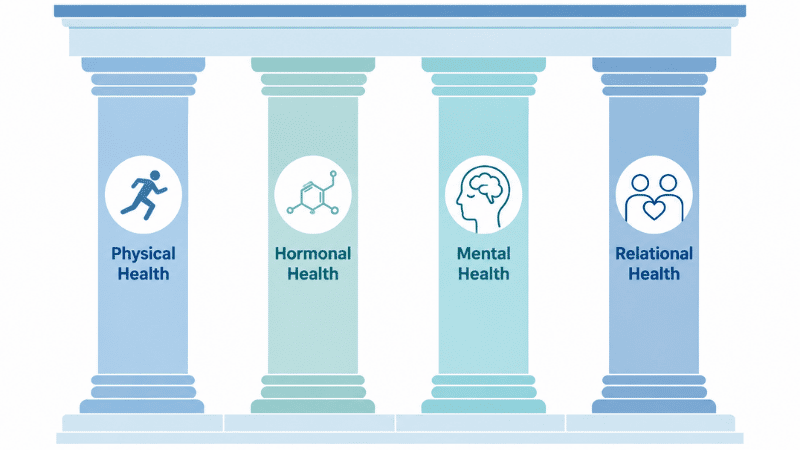
Physical Health
The physical dimension of men’s sexual health includes reproductive anatomy, hormonal balance, cardiovascular function, and the presence or absence of infections or chronic conditions.
Cardiovascular health plays a central role in erectile function. Erections depend on healthy blood flow, which means that conditions affecting the heart and blood vessels — including high blood pressure, high cholesterol, and type 2 diabetes — frequently manifest first as changes in sexual function. In clinical practice, erectile difficulties in men under 50 are sometimes the earliest indicator of underlying vascular disease, making them worth investigating rather than dismissing.
The pelvic floor — a group of muscles supporting the bladder, bowel, and sexual function — is frequently overlooked in men’s health conversations. Pelvic floor dysfunction, which can result from sedentary habits, chronic tension, or prostate issues, is an underrecognized contributor to both premature ejaculation and erectile difficulties.
Hormonal Health
Testosterone is the primary male sex hormone, and its levels naturally decline after age 30 at approximately 1–2% per year. This decline is gradual and does not cause sudden changes in most men. However, a significant drop — known clinically as hypogonadism — is a diagnosable and treatable condition, distinct from the normal aging process.
Beyond testosterone, other hormones matter considerably. Chronic stress elevates cortisol levels, which directly suppresses testosterone production. Thyroid dysfunction — both overactive and underactive — can significantly affect libido, energy, and sexual function in men, yet it is frequently overlooked in routine health conversations.
Mental and Emotional Health
The relationship between mental health and sexual health in men is bidirectional and well-documented. Depression is associated with reduced libido and diminished sexual satisfaction. Performance anxiety is one of the most common contributors to erectile difficulties in men under 40. Chronic stress affects hormonal balance, sleep quality, and relationship dynamics — all of which influence sexual function directly.
Despite this, men are significantly less likely than women to seek mental health support, and performance anxiety in particular is often endured quietly rather than addressed. Recognizing that mental health and sexual health are interconnected is not a concession — it is a clinical reality that opens up effective avenues for treatment.
Relational Health
Sexual health does not exist in isolation — it lives inside relationships and communication patterns. Research consistently shows that couples who communicate openly about sexual health report better sexual outcomes and greater relationship satisfaction overall.
This includes conversations about STI status and testing, contraceptive decisions, changes in desire or function over time, and any physical concerns that arise. These conversations can feel uncomfortable at first. They become easier with practice — and the evidence suggests they are worth having.
What Is Normal at Different Life Stages
Men’s sexual health changes across decades in predictable ways. Understanding these changes prevents unnecessary alarm and helps distinguish normal variation from conditions that warrant medical attention.
Men’s Sexual Health in Your 20s
The 20s are generally characterized by peak testosterone levels and high erectile reliability. However, this decade carries specific risks: STI rates are highest among young adults, and performance anxiety — often rooted in unrealistic expectations — is common and frequently goes unaddressed.
What’s normal: Variation in desire and arousal from week to week. Occasional difficulty with erections due to stress, alcohol, or fatigue. Rapid ejaculation, which is common in younger men and often improves with awareness and time.
Worth discussing with a doctor: Persistent erectile difficulties unrelated to lifestyle factors. Any symptoms of a sexually transmitted infection, including unusual discharge, sores, or pain during urination. Significant, unexplained changes in libido lasting more than a few weeks.
Men’s Sexual Health in Your 30s
Testosterone levels begin their gradual decline in the mid-30s, though most men will not notice meaningful changes during this decade. Career pressure, relationship transitions, and reduced sleep quality are common contributors to decreased libido and emerging sexual health concerns during this period.
What’s normal: A modest reduction in spontaneous sexual desire compared to the early 20s. Slightly longer time needed to achieve erection. Greater awareness of how stress and poor sleep affect sexual function.
Worth discussing with a doctor: Erectile difficulties occurring consistently rather than situationally. Significant fatigue combined with reduced libido and mood changes, which may indicate low testosterone or thyroid dysfunction. Any fertility concerns.
Men’s Sexual Health in Your 40s and Beyond
By the 40s, hormonal changes become more noticeable for some men. Prostate health becomes an active area of monitoring. Cardiovascular health — which directly affects erectile function — becomes increasingly relevant as a long-term investment in sexual well-being.
What’s normal: A gradual reduction in spontaneous erections. A longer refractory period between sexual encounters. Some reduction in ejaculatory force.
Worth discussing with a doctor: Erectile dysfunction occurring consistently and affecting quality of life — this is treatable, not inevitable. Lower urinary tract symptoms, including difficulty initiating urination or increased nighttime frequency. Any new lumps, changes in testicular size, or genital pain, which require prompt evaluation.
Common Men’s Sexual Health Problems: What You Should Know
Premature Ejaculation
Premature ejaculation (PE) is defined clinically as ejaculation occurring within approximately one minute of penetration, causing personal distress, and happening consistently rather than occasionally. It is the most common male sexual dysfunction, affecting an estimated 20–30% of men at some point in their lives.
PE has both biological and psychological components, and it responds well to treatment. Behavioral techniques — including the stop-start method and the squeeze technique — have a strong evidence base. Pelvic floor physical therapy is increasingly recognized as an effective clinical intervention. For persistent cases, topical anesthetic agents and certain prescription medications are available through a physician.
If rapid ejaculation has been a consistent concern and self-directed approaches have not helped, a clinical evaluation is a reasonable and productive next step — not a last resort.
→ Related: Premature Ejaculation: Causes, Facts, and Evidence-Based Solutions
Erectile Dysfunction
Erectile dysfunction (ED) — defined as the consistent inability to achieve or maintain an erection sufficient for satisfactory sexual activity — affects an estimated 30 million men in the United States, according to the National Institute of Diabetes and Digestive and Kidney Diseases. It becomes more prevalent with age, but it is not an inevitable consequence of getting older.
A clinically important distinction: ED in men under 40 is often primarily psychological in origin, while ED in men over 50 more frequently has an underlying physical component — including cardiovascular or hormonal factors — that warrants investigation. In either case, effective treatment options exist.
→ Related: Erectile Dysfunction: A Clinical Overview for Men of All Ages
Low Libido in Men
A reduction in sexual desire is among the most common and most frequently dismissed men’s sexual health concerns. Its causes are numerous and often overlapping: low testosterone, depression, chronic stress, relationship dissatisfaction, medication side effects, sleep deprivation, and obesity all contribute independently and in combination.
Because libido is affected by so many intersecting factors, identifying the primary driver — whether hormonal, psychological, lifestyle-related, or relational — is more effective than applying generic solutions. A physician can help distinguish between these causes through targeted evaluation.
Sexually Transmitted Infections in Men
Men are at risk for the full range of STIs, including chlamydia, gonorrhea, syphilis, herpes (HSV), human papillomavirus (HPV), and HIV. Several of these — chlamydia and gonorrhea in particular — frequently produce no symptoms in men.
According to the Centers for Disease Control and Prevention (CDC), chlamydia is the most commonly reported STI in the United States, and the majority of infected men experience no noticeable symptoms. This makes routine testing the only reliable means of knowing your status with confidence — not just a precaution for high-risk situations.
→ Related: STI Testing: When, Where, and What to Expect
How to Improve Men’s Sexual Health: Evidence-Based Steps
Prioritize Cardiovascular Fitness
Because erectile function is a direct reflection of vascular health, cardiovascular fitness is the single most impactful investment most men can make in their long-term sexual health. Regular aerobic exercise, a diet low in processed foods and saturated fats, not smoking, and managing blood pressure and cholesterol all protect erectile function as men age.
The evidence is consistent: men who exercise regularly report significantly better erectile function than sedentary men of equivalent age. The standard clinical recommendation of 150 minutes of moderate-intensity aerobic activity per week is not arbitrary — it is the threshold at which meaningful cardiovascular and sexual health benefits are reliably observed.
If you only have 10 minutes: A brisk 10-minute walk still activates cardiovascular benefit. The goal is daily movement, not perfect workouts. Start where you are.
Protect Sleep Quality
Testosterone production occurs primarily during deep sleep. Chronic sleep deprivation — consistently fewer than seven hours per night — measurably reduces testosterone levels and negatively affects libido, mood, and cognitive function. Untreated obstructive sleep apnea is associated with significantly lower testosterone levels and sexual dysfunction, and it is far more prevalent than most men recognize.
If you snore regularly, wake frequently during the night, or feel persistently fatigued despite adequate hours in bed, a sleep evaluation is a worthwhile next step.
Treat Stress as a Medical Issue, Not a Character Trait
Chronic psychological stress is not a background condition to accept — it is a physiological state with measurable hormonal consequences. Sustained elevated cortisol directly suppresses testosterone production and reduces sexual desire. This is a biological mechanism, not a personal failing.
Stress management strategies with a consistent clinical evidence base include regular aerobic exercise, mindfulness-based practices, adequate sleep, and in many cases, professional psychological support. If chronic stress is persistently affecting your quality of life, addressing it is a health decision — not an optional one.
If you’ve tried and it’s not improving: Persistent stress symptoms that don’t respond to lifestyle adjustment may indicate anxiety, depression, or burnout — all of which are diagnosable and treatable conditions. A clinical conversation is the appropriate next step.
Get Tested on a Regular Schedule
Routine STI testing is a standard component of adult healthcare, not an admission of unusual risk. Many men delay testing because they assume it is only necessary after a specific concerning event. In practice, because many STIs produce no symptoms, regular screening is the only way to know your status.
If you are sexually active, an annual sexual health screen is the clinical minimum. More frequent testing — every three to six months — is advisable for men with multiple partners or those who have sex with men, in alignment with CDC guidelines.
Limit Alcohol and Eliminate Tobacco
Alcohol is a physiological depressant that reduces testosterone levels and impairs erectile function at higher doses. Regular heavy drinking is clearly associated with long-term sexual dysfunction. Moderate consumption — up to two standard drinks per day — has not been conclusively linked to permanent impairment, but its short-term effects on erectile function are well-established.
Tobacco smoking is an independent risk factor for erectile dysfunction, due to direct and progressive damage to blood vessel walls. The relationship is dose-dependent: greater smoking history correlates with greater erectile risk. This is one of the most straightforward modifiable risk factors for long-term men’s sexual health.
Warning Signs: When to See a Doctor About Men’s Sexual Health
The following situations warrant professional evaluation rather than continued self-management:
- Erectile difficulties occurring consistently and causing personal distress, regardless of age
- A noticeable, unexplained decline in sexual desire lasting more than four to six weeks
- Any unusual genital symptoms — discharge, sores, pain during urination, or unexplained lumps
- Significant changes in urinary habits, particularly difficulty initiating urination or increased frequency at night
- Psychological distress related to sexual function that is affecting daily life or close relationships
- Concerns about STI exposure, even in the absence of symptoms
These are routine conversations in clinical practice. A family physician, urologist, or sexual health specialist encounters them regularly. The discomfort is almost always one-sided — and it fades quickly.
Frequently Asked Questions About Men’s Sexual Health
What are the most common men’s sexual health problems? The most common concerns include premature ejaculation, erectile dysfunction, low libido, and sexually transmitted infections. PE is the most prevalent male sexual dysfunction overall. ED becomes increasingly common with age but is not inevitable. Low libido is frequently tied to hormonal, psychological, or lifestyle factors and is often addressable once the primary cause is identified.
At what age does men’s sexual health typically start to change? Testosterone levels begin declining gradually around age 30, at approximately 1–2% per year. Most men notice more meaningful changes in their 40s, including slower arousal, longer refractory periods, and some reduction in spontaneous desire. These changes are normal — what matters is distinguishing gradual variation from symptoms that indicate an underlying, treatable condition.
How often should men get tested for STIs? Sexually active adults with new or multiple partners should get tested at minimum once per year. Men who have sex with men are advised to test every three to six months, in line with CDC recommendations. Many STIs are asymptomatic in men, making regular screening the only reliable means of knowing your status.
Can stress really cause erectile dysfunction? Yes. Chronic stress elevates cortisol levels, which suppresses testosterone production and can interfere with the hormonal and vascular mechanisms needed for erection. Performance anxiety — a specific form of psychological stress — is one of the most common causes of erectile difficulties in men under 40. Addressing the underlying stress often significantly improves erectile function.
Is low testosterone the same as low libido? Not necessarily. While low testosterone (hypogonadism) is one cause of reduced sexual desire, low libido in men can also result from depression, chronic stress, relationship difficulties, medication side effects, sleep deprivation, and other factors. A blood test can measure testosterone levels, but resolving low libido effectively often requires identifying which factor — or combination of factors — is actually driving it.
What lifestyle changes have the greatest impact on men’s sexual health? The evidence most consistently supports regular aerobic exercise, adequate sleep, not smoking, moderate alcohol consumption, and effective stress management. Cardiovascular fitness in particular has a direct and measurable impact on erectile function. These are not generic wellness suggestions — they address specific biological mechanisms that affect men’s sexual health.
When should erectile dysfunction be evaluated medically? ED warrants medical evaluation when it occurs consistently rather than occasionally, causes personal distress, and is not clearly linked to situational factors such as alcohol use or acute stress. ED in men under 40 should not be dismissed as psychological without proper evaluation. ED in men over 50 warrants investigation for underlying cardiovascular or hormonal causes.
The Bottom Line: Taking Men’s Sexual Health Seriously
Men’s sexual health is a legitimate and important dimension of overall well-being — one that deserves the same attentive, matter-of-fact approach as cardiovascular health, sleep quality, or mental fitness.
The most significant barriers to good sexual health in men are rarely biological. They are the reluctance to seek information, discomfort with clinical conversations, and the quiet acceptance of dysfunction as something inevitable or not worth addressing. None of those barriers are fixed.
Understanding your body, recognizing meaningful changes, getting tested regularly, and seeking professional input when something concerns you — these are the practical foundations of maintaining men’s sexual health across a lifetime. They are straightforward steps that most men, with the right information, are fully capable of taking.
References
- World Health Organization. Sexual Health. https://www.who.int/health-topics/sexual-health
- Centers for Disease Control and Prevention. Sexually Transmitted Infections Surveillance, 2022. https://www.cdc.gov/std/statistics
- National Institute of Diabetes and Digestive and Kidney Diseases. Erectile Dysfunction. https://www.niddk.nih.gov/health-information/urologic-diseases/erectile-dysfunction
- Feldman HA, et al. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. Journal of Urology. 1994;151(1):54–61.
- Traish AM, et al. The dark side of testosterone deficiency. Journal of Andrology. 2009;30(1):10–22.