There is a particular kind of frustration that many women know well: sitting in a doctor’s office, trying to explain something that feels genuinely wrong with your body, and being told it is probably just stress. Or hormones. Or something you need to simply live with.
That experience — of not being fully heard, of leaving with more questions than answers — is part of why so many women turn to the internet at 11 PM, searching for explanations their appointments never provided. If you are here for that reason, this guide is for you.
What follows is a medically grounded, plainly written overview of women’s reproductive health: what it encompasses, what changes are expected across different life stages, which symptoms deserve professional attention, and what the evidence actually supports when it comes to protecting your long-term well-being. No dismissiveness, no vague reassurances, and no unnecessary alarm.
Key Takeaways
- Women’s reproductive health spans physical, hormonal, mental, and relational dimensions — and changes meaningfully across different life stages, from the early 20s through perimenopause and beyond.
- According to the National Institutes of Health, reproductive disorders affect millions of American women each year, yet many go undiagnosed for years due to normalization of symptoms.
- Estrogen and progesterone fluctuate cyclically throughout the menstrual cycle and decline significantly during perimenopause — changes that directly affect libido, mood, sleep, and vaginal health.
- Low libido in women is the most commonly reported female sexual concern, affecting an estimated 10–15% of women across all age groups. It is almost always multifactorial and often highly treatable.
- Routine gynecological care — including cervical screening, STI testing, and hormonal evaluation — is the foundation of long-term reproductive health, not a resource reserved for when something feels wrong.
What Women’s Reproductive Health Actually Means
Women’s reproductive health is a term that tends to be used narrowly — reduced to pregnancy, contraception, or STI prevention — when in reality it encompasses considerably more. The World Health Organization defines reproductive health as a state of complete physical, mental, and social well-being in all matters relating to the reproductive system, not merely the absence of disease or infirmity.
In practice, this means understanding how your menstrual cycle works and what variations are normal for your body. It means recognizing how hormonal fluctuations affect mood, energy, libido, and physical comfort throughout the month. It means having access to clear, accurate information about contraception, fertility, and the changes that come with age — without shame, and without having to advocate aggressively for basic care.
Women’s reproductive health is not a static condition. It evolves through distinct phases — adolescence, the reproductive years, perimenopause, and menopause — each with its own hormonal landscape, its own common concerns, and its own preventive priorities. Understanding where you are in that landscape is the starting point for taking care of yourself well.
The Hormonal Foundation of Women’s Reproductive Health
How Estrogen and Progesterone Shape Your Health
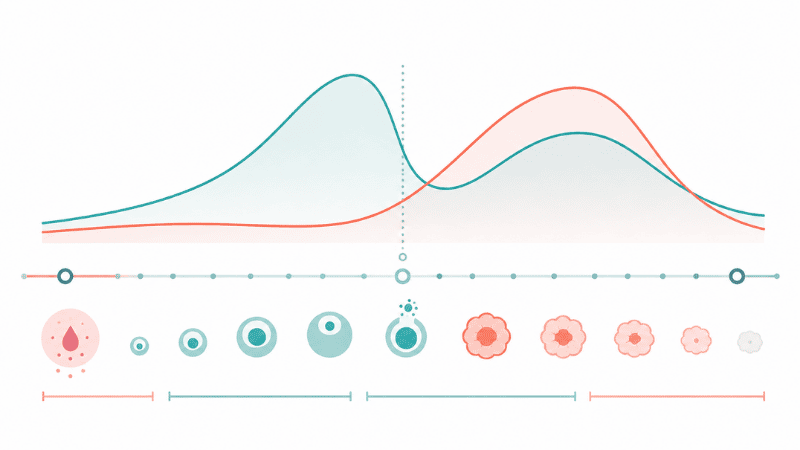
The female reproductive system is governed by a hormonal axis involving the hypothalamus, the pituitary gland, and the ovaries — a system that coordinates the menstrual cycle, ovulation, and the preparation of the uterine lining each month.
Two hormones sit at the center of this system: estrogen and progesterone. Estrogen, primarily in the form of estradiol during the reproductive years, drives the first half of the menstrual cycle, supports vaginal lubrication, maintains bone density, and influences mood and cognitive function. Progesterone dominates the second half of the cycle, following ovulation, preparing the uterine lining and — when levels drop — triggering menstruation.
These hormones do not operate in isolation. They interact with cortisol, thyroid hormones, insulin, and neurotransmitters including serotonin and dopamine. This is why hormonal imbalances rarely produce a single isolated symptom — they tend to produce constellations of effects across mood, energy, sleep, libido, and physical comfort simultaneously.
What Disrupts Hormonal Balance
Several factors can disrupt the hormonal axis that governs women’s reproductive health:
- Chronic psychological stress elevates cortisol, which interferes with the hormonal signaling that regulates the menstrual cycle. This is one of the reasons that significant stress can delay or alter periods.
- Significant changes in body weight — both loss and gain — affect estrogen production and can disrupt ovulation.
- Thyroid dysfunction, both hypothyroidism and hyperthyroidism, directly affects menstrual regularity, fertility, libido, and overall energy. It is estimated that thyroid disorders affect women at five to eight times the rate of men, and they are frequently underdiagnosed.
- Polycystic ovary syndrome (PCOS), one of the most common endocrine disorders in women of reproductive age, involves elevated androgen levels and disrupted ovulation — producing effects on the menstrual cycle, fertility, skin, and metabolic health.
Understanding these connections is not meant to be alarming. It is meant to be useful — because symptoms that feel disconnected often share a hormonal root cause that a physician can identify and address.
Women’s Reproductive Health Across Different Life Stages
In Your 20s: Establishing Your Baseline
The 20s are typically the peak of hormonal regularity for most women, but they are also the decade when many conditions — including PCOS, endometriosis, and thyroid dysfunction — first become apparent. They are also the period of highest STI risk, with chlamydia rates peaking in women aged 15–24 according to the Centers for Disease Control and Prevention.
What is normal: Some variation in cycle length from month to month, particularly in the early 20s. Mild cramping before and during menstruation. Changes in libido across the menstrual cycle, which reflects normal hormonal fluctuation — desire often peaks around ovulation and decreases in the luteal phase.
Worth discussing with a doctor: Periods that are consistently very painful and disrupt daily function — this is not a normal baseline to accept, and may indicate endometriosis or another treatable condition. Cycles that are consistently irregular or absent. Any symptoms of an STI, including unusual discharge, pelvic pain, or discomfort during urination. Significant and persistent changes in mood that align with the menstrual cycle, which may indicate premenstrual dysphoric disorder (PMDD).
In Your 30s: Navigating Shifting Priorities
For many women, the 30s bring significant life changes — career demands, relationship transitions, decisions about fertility — alongside the earliest, often subtle shifts in hormonal patterns. Fertility begins to decline gradually after age 32 and more noticeably after 37, though this varies considerably between individuals.
Libido in this decade is frequently affected by factors that have little to do with hormones directly: chronic sleep deprivation, high occupational stress, relationship satisfaction, and the psychological weight of managing competing responsibilities. These are real contributors to sexual well-being and deserve to be addressed as such.
What is normal: A gradual shift in the quality of the menstrual cycle as the decade progresses. Some women notice changes in flow, duration, or premenstrual symptoms. Variation in libido that correlates with life stress rather than the menstrual cycle.
Worth discussing with a doctor: Any new onset of irregular cycles after years of regularity, which may warrant hormonal evaluation. Persistent pelvic pain, which may indicate fibroids — benign uterine growths that are most common in women in their 30s and 40s. Fertility concerns if conception has not occurred after 12 months of trying, or after six months for women over 35.
In Your 40s and Beyond: Perimenopause and the Hormonal Transition
Perimenopause — the transitional phase before menopause — typically begins in the mid-to-late 40s, though it can start earlier. It is defined by fluctuating and eventually declining estrogen levels, and it produces a range of effects that many women are not adequately prepared for.
Common perimenopausal changes include irregular menstrual cycles, vasomotor symptoms (hot flashes and night sweats), sleep disruption, mood changes, reduced vaginal lubrication, and changes in libido. These are physiological responses to hormonal transition, not psychological weakness or inevitable decline.
The genitourinary syndrome of menopause (GSM) — a clinical term for the vaginal dryness, discomfort, and urinary changes associated with declining estrogen — affects an estimated 50% of postmenopausal women, yet fewer than 25% seek treatment, often because they are not aware that effective, safe options exist.
What is normal: Cycle irregularity beginning in the mid-to-late 40s. Changes in flow intensity. Vasomotor symptoms. Shifts in libido and vaginal comfort.
Worth discussing with a doctor: Vasomotor symptoms that are significantly disrupting sleep or quality of life — hormone therapy and non-hormonal options are available and effective. Vaginal dryness or discomfort during sex that is affecting your well-being — this is medically addressable. Any postmenopausal bleeding, which always requires evaluation.
Common Women’s Sexual Health Concerns
Low Libido in Women
Reduced sexual desire is the most commonly reported female sexual health concern across all age groups. Unlike in men, where libido is primarily driven by testosterone, women’s sexual desire is influenced by a more complex interaction of hormones, emotional context, relationship quality, physical comfort, stress, and past experience.
The medical classification distinguishes between hypoactive sexual desire disorder (HSDD) — persistent, distressing low desire that is not explained by another condition or relationship factor — and situational low desire, which has an identifiable contextual cause. Both are worth addressing, but through different pathways.
Common contributing factors include hormonal changes (particularly declining estrogen and testosterone), untreated depression or anxiety, certain medications (including some antidepressants and hormonal contraceptives), chronic pain, relationship dissatisfaction, and unresolved psychological history. Identifying which factor — or combination of factors — is driving the concern is the starting point for effective care.
If lifestyle changes have not helped: Persistent low libido that is causing distress and has not responded to sleep improvement, stress reduction, or relationship communication warrants a clinical evaluation. Hormonal testing, a medication review, and in some cases psychological support or sex therapy are all evidence-based options.
→ Related: Low Libido in Women: Causes, Hormones, and When to Seek Help
Vaginal Dryness and Discomfort
Vaginal dryness — insufficient natural lubrication — is most commonly associated with the hormonal changes of perimenopause and menopause, but it can occur at any age. Contributing factors include certain hormonal contraceptives, antihistamines, antidepressants, breastfeeding, and inadequate arousal time.
When vaginal dryness causes discomfort during sexual activity — a condition clinically termed dyspareunia — it is both physically and psychologically significant. It frequently contributes to reduced sexual desire and avoidance, creating a cycle that can be effectively interrupted with appropriate treatment.
Effective options include vaginal moisturizers for daily use, lubricants for use during sexual activity, and — for perimenopausal and postmenopausal women — low-dose vaginal estrogen, which addresses the underlying hormonal cause rather than just the symptoms. A gynecologist can help identify which approach is most appropriate for your situation.
Painful Sex (Dyspareunia)
Pain during or after sexual intercourse is not a normal baseline to accept. It has multiple potential causes — including vaginal dryness, vaginismus (involuntary pelvic floor muscle tension), endometriosis, pelvic inflammatory disease, vulvodynia, and ovarian cysts — many of which are diagnosable and treatable.
Despite its prevalence — affecting an estimated 10–20% of women at some point — dyspareunia is significantly underreported. Many women do not raise it with their healthcare provider, assuming it is something to manage privately rather than a clinical concern. It is a clinical concern, and it deserves evaluation.
→ Related: Painful Sex: Causes, Diagnosis, and What to Do Next
Sexually Transmitted Infections in Women
Women are at risk for the same range of STIs as men, but the consequences of certain infections — particularly chlamydia and gonorrhea — can be more significant in women if untreated, as they can lead to pelvic inflammatory disease (PID) and, in some cases, affect fertility.
As with men, many STIs produce no symptoms in women. The CDC recommends annual chlamydia and gonorrhea screening for all sexually active women under 25, and for older women with new or multiple sexual partners. HPV screening through routine cervical testing (Pap smear and HPV co-test) is a cornerstone of women’s reproductive health care.
→ Related: STI Testing: When, Where, and What to Expect
How to Maintain Women’s Sexual Wellness: Evidence-Based Priorities
Know Your Menstrual Cycle
Familiarity with your own cycle — its length, regularity, flow characteristics, and how you feel at different phases — is a genuinely useful health tool, not just a fertility planning strategy. Significant deviations from your established baseline are often the first signal of hormonal changes, thyroid dysfunction, or other conditions worth evaluating.
Cycle tracking, whether through a simple calendar or a dedicated application, provides the kind of longitudinal data that makes clinical conversations more productive. It answers questions your doctor will ask and helps you distinguish normal variation from a meaningful change.
Prioritize Sleep as a Hormonal Health Issue
Sleep is not a lifestyle preference — it is a physiological necessity with direct hormonal consequences. Chronic sleep deprivation disrupts the hypothalamic-pituitary axis that regulates reproductive hormones, affects cortisol levels, and is associated with increased menstrual irregularity and reduced libido.
For women in perimenopause, where night sweats and sleep disruption are common, addressing sleep quality is a medical priority. If vasomotor symptoms are significantly disrupting sleep, this warrants a clinical conversation about management options.
If 10 minutes is all you have: Consistent sleep and wake times — even on weekends — are the single most impactful sleep habit for hormonal regulation. Start there before addressing anything else.
Manage Stress With the Same Attention You’d Give a Physical Symptom
The hormonal consequences of chronic stress in women are well-documented. Elevated cortisol suppresses the hormonal signals that regulate ovulation, affects thyroid function, and reduces sexual desire. Many women recognize intellectually that stress is affecting their health but continue to treat it as a background condition rather than something requiring active management.
Stress management strategies with clinical evidence behind them include regular aerobic exercise, mindfulness-based practices, adequate sleep, and professional psychological support where appropriate. If stress has become persistent and is affecting your menstrual cycle, libido, or overall quality of life, it deserves the same clinical attention as any other symptom.
Attend Routine Gynecological Care
Routine gynecological care is not just for when something feels wrong. It is the system through which early-stage conditions — including cervical cell changes, asymptomatic STIs, and hormonal imbalances — are identified before they become more complex problems.
Current clinical guidelines recommend:
- Cervical screening (Pap smear) beginning at age 21, with frequency depending on age and results
- Annual chlamydia and gonorrhea testing for sexually active women under 25
- STI testing based on individual risk factors for women 25 and older
- Breast self-awareness and clinical evaluation as recommended by your provider
Finding a gynecologist or sexual health provider with whom you feel comfortable communicating openly is worth the investment of time. The quality of your clinical conversations directly affects the quality of your care.
Warning Signs: When to Seek Medical Attention
The following warrant professional evaluation rather than continued self-management or waiting to see if things improve:
- Menstrual cycles that are consistently very painful, lasting beyond the first one to two days, or significantly disrupting daily functioning
- Unexplained pelvic pain, particularly if persistent or associated with fever
- Any pain during sexual intercourse that is new, worsening, or consistent
- Unusual vaginal discharge — changes in color, odor, or consistency from your established baseline
- Significant changes in menstrual regularity after a period of consistency
- A noticeable, persistent decline in sexual desire that is causing personal distress
- Any postmenopausal vaginal bleeding
- Symptoms of a possible STI, including burning during urination, unusual sores, or pelvic discomfort
None of these are reasons for alarm before evaluation. They are reasons to make an appointment.
Frequently Asked Questions
What is considered normal for women’s reproductive health? Normal varies considerably between individuals, which is why establishing your own baseline matters more than comparing yourself to an average. In general, a menstrual cycle lasting between 21 and 35 days, mild to moderate cramping, and variation in libido across the cycle are within normal parameters. What falls outside your individual normal — persistent pain, significant irregularity, unexplained changes — is worth discussing with a physician.
What are the most common women’s reproductive health concerns? The most commonly reported concerns include menstrual irregularity, painful periods, low libido, vaginal dryness and discomfort, pain during sex, and symptoms related to hormonal changes including perimenopause. Many of these overlap and share underlying hormonal or psychological causes.
How does age affect women’s sexual health? Women’s reproductive health shifts meaningfully across decades. The 20s typically bring hormonal regularity alongside higher STI risk. The 30s often involve the effects of life stress and early hormonal shifts on libido and cycle quality. The 40s introduce perimenopause — with its characteristic cycle changes, vasomotor symptoms, and shifts in vaginal health. Each stage has its own concerns and its own opportunities for proactive care.
What causes low libido in women? Low libido in women is almost always multifactorial. Common contributors include hormonal changes (particularly declining estrogen and testosterone), depression and anxiety, chronic stress, sleep deprivation, certain medications, relationship dissatisfaction, pain during sex, and psychological history. Identifying the primary driver — through a clinical evaluation if necessary — is more effective than generic interventions.
Is vaginal dryness only a menopausal issue? No. While vaginal dryness is most commonly associated with the estrogen decline of perimenopause and menopause, it can occur at any age. Certain hormonal contraceptives, antihistamines, antidepressants, breastfeeding, and insufficient arousal can all contribute. Effective treatment options exist for all age groups.
How often should women get tested for STIs? Annual chlamydia and gonorrhea screening is recommended for all sexually active women under 25. For women 25 and older, testing frequency depends on individual risk factors including number of partners and partner STI history. Cervical screening (Pap smear) should begin at age 21, with frequency determined by results and age. Because many STIs produce no symptoms in women, routine screening is the only reliable means of knowing your status.
When should I see a doctor about menstrual pain? Menstrual discomfort that responds to standard over-the-counter pain relief and does not significantly disrupt daily functioning is generally within the range of normal. Pain that is severe, persists beyond the first two days of menstruation, does not respond to standard analgesia, or is accompanied by heavy bleeding warrants evaluation — it may indicate endometriosis, fibroids, or another treatable condition.
The Bottom Line
Women’s reproductive health is a broad, nuanced, and important dimension of overall well-being — one that spans hormones, menstrual health, sexual wellness, preventive care, and the changes that come with every decade of life.
The most persistent barrier to good reproductive health in women is not access to information alone, but the accumulated experience of not being taken seriously. Of symptoms being normalized, minimized, or attributed to stress. Of leaving appointments without answers.
Understanding your body, tracking meaningful changes, attending routine care, and advocating clearly for clinical evaluation when something concerns you — these are not small acts. They are the foundation of maintaining your women’s reproductive health across a lifetime, on your own terms.
References
- World Health Organization. Reproductive Health. https://www.who.int/health-topics/sexual-and-reproductive-health
- National Institute of Environmental Health Sciences. Reproductive Health. https://www.niehs.nih.gov/health/topics/conditions/repro-health
- Centers for Disease Control and Prevention. Sexually Transmitted Infections Surveillance, 2022. https://www.cdc.gov/std/statistics
- National Institutes of Health, National Library of Medicine. The Biological Basis for Women’s Health Through the Lens of Chromosomes and Hormones. https://www.ncbi.nlm.nih.gov/books/NBK612390/
- Shifren JL, et al. Sexual problems and distress in United States women. Obstetrics & Gynecology. 2008;112(5):970–978.
Related Articles on PureInti
- Low Libido in Women: Causes, Hormones, and When to Seek Help
- Painful Sex: Causes, Diagnosis, and What to Do Next
- STI Testing: When, Where, and What to Expect
- How to Talk to Your Partner About Sexual Health
- Men’s Sexual Health: A Complete Guide for Adults