You are tired in a way that sleep does not fix. Your motivation has dipped. The interest in intimacy that used to feel natural now requires an effort you cannot quite explain. You have mentioned it to a doctor and been told your thyroid is fine, your iron levels are normal, and perhaps you should try to manage your stress better.
What may not have been checked — or even mentioned — is your testosterone level.
Testosterone is almost exclusively discussed in the context of men’s health, which is why its role in women’s physiology is so consistently overlooked. But testosterone is produced by women’s ovaries and adrenal glands throughout life, and it plays a direct role in sexual desire, energy, muscle tone, mood, bone health, and cognitive function. When levels fall below the range that supports normal function, the symptoms are real, measurable, and frequently attributed to everything else first.
This guide explains what low testosterone in women actually looks like, what causes it, how it is diagnosed, and what evidence-based options exist for addressing it.
Key Takeaways
- Testosterone is produced by the ovaries and adrenal glands in women and plays a direct role in libido, energy, muscle tone, mood, and bone density — not just in men.
- Women’s testosterone levels decline gradually from the 20s onward, with a significant drop during perimenopause and menopause. By menopause, testosterone levels may be half of what they were at peak.
- The symptoms of low testosterone in women — fatigue, reduced libido, low mood, muscle weakness — are non-specific and frequently attributed to stress, depression, thyroid issues, or simply aging before testosterone is evaluated.
- A blood test measuring total and free testosterone, ideally performed in the morning when levels are highest, is the only reliable means of diagnosis. Normal ranges for women are significantly lower than for men and vary by age and laboratory.
- Testosterone therapy for women remains off-label in many countries but has a growing evidence base, particularly for postmenopausal women with low libido. Lifestyle interventions including resistance training, sleep optimization, and stress management also support healthy testosterone levels.
What Is Testosterone and Why Do Women Need It
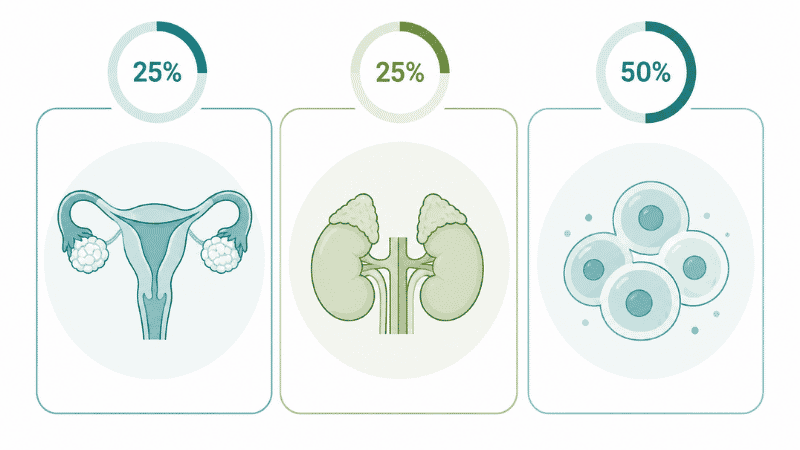
Testosterone is classified as an androgen — a group of hormones traditionally associated with male physiology — but it is produced in meaningful quantities in women throughout life. Women’s ovaries produce approximately 25% of their testosterone; the adrenal glands produce another 25%; and the remaining 50% is produced through conversion of other hormones in peripheral tissues.
In women, testosterone contributes to:
Sexual desire and arousal — Testosterone is the primary hormonal driver of libido in both sexes. Declining testosterone is one of the most consistent hormonal contributors to reduced sexual desire in women, independently of estrogen levels.
Energy and physical vitality — Testosterone supports mitochondrial function and contributes to the physical energy and endurance that most people associate with overall well-being. Women with low testosterone frequently report a specific kind of fatigue — not sleepiness, but a lack of drive and physical resilience.
Muscle mass and bone density — Testosterone is anabolic, meaning it supports the building and maintenance of lean muscle tissue. It also contributes to bone density alongside estrogen, making it relevant to osteoporosis risk as women age.
Mood and cognitive function — Testosterone receptors are present throughout the brain. Low testosterone in women is associated with low mood, reduced motivation, cognitive fog, and in some cases, depressive symptoms — though the relationship is complex and bidirectional.
Menstrual cycle and fertility — Testosterone plays a role in the hormonal cascade that governs ovulation, and imbalances — both high and low — can affect cycle regularity and fertility.
Women’s Testosterone Levels: What Is Normal
Understanding what constitutes normal testosterone levels in women requires more nuance than the question suggests, because normal ranges vary significantly by age, reproductive stage, and the laboratory method used.
In general terms, total testosterone in women typically falls between 15 and 70 nanograms per deciliter (ng/dL), compared to 300–1,000 ng/dL in men. Peak levels occur in the early to mid-20s and decline gradually thereafter.
By menopause, testosterone levels may have fallen to approximately 50% of their peak value. Women who have had their ovaries surgically removed (oophorectomy) experience a more rapid and pronounced decline, as the ovaries are the primary source of testosterone in premenopausal women.
Two measurements are clinically relevant:
Total testosterone — measures all testosterone in the bloodstream, including that bound to proteins.
Free testosterone — measures the testosterone that is biologically active and available to cells. This is often the more clinically meaningful figure, as testosterone bound to sex hormone-binding globulin (SHBG) is not available for use by tissues.
Testing is ideally performed in the morning, when testosterone levels are at their daily peak. A single measurement may not be sufficient for diagnosis, as levels fluctuate throughout the menstrual cycle.
Symptoms of Low Testosterone in Women: What to Look For
The symptoms of low testosterone in women are notoriously non-specific — meaning they overlap substantially with symptoms of other conditions including thyroid dysfunction, iron deficiency, depression, and the hormonal changes of perimenopause. This overlap is the primary reason low testosterone is so frequently missed or attributed elsewhere.
The Most Commonly Reported Symptoms
Reduced sexual desire — the most consistently documented symptom of low testosterone in women. This is often described not as an aversion to intimacy, but as an absence of spontaneous desire — the interest that used to arise naturally has simply become quieter or absent.
Persistent fatigue and low energy — a specific quality of fatigue that is not resolved by adequate sleep. Women with low testosterone often describe feeling physically depleted, lacking the resilience and drive that characterized their earlier years.
Reduced muscle tone and strength — testosterone supports lean muscle maintenance. Women with low levels may notice that maintaining muscle mass has become harder despite consistent exercise, or that they feel physically weaker than they previously did.
Low mood and reduced motivation — not necessarily clinical depression, but a flattening of the motivational drive that makes everyday tasks feel heavier. Some women describe it as a loss of the “spark” that used to characterize their engagement with life.
Cognitive changes — difficulty concentrating, brain fog, and reduced mental sharpness are reported by some women with low testosterone, though the research on this association is less definitive than for the symptoms above.
Vaginal dryness and thinning — testosterone contributes to the health of vaginal tissue alongside estrogen. Low levels can compound the vaginal dryness associated with declining estrogen, particularly in perimenopause.
Thinning hair and changes in skin quality — some women notice hair thinning or changes in skin texture alongside other low testosterone symptoms, though these are less specific indicators.
Signs of Low Testosterone in Women vs Other Conditions
The challenge in diagnosing low testosterone in women is that its symptoms are indistinguishable from those of several other conditions without a blood test. The following overlap significantly:
- Thyroid dysfunction — particularly hypothyroidism, which produces fatigue, low mood, cognitive fog, and reduced libido. A thyroid panel should be included in any hormonal evaluation.
- Iron deficiency anemia — produces fatigue and reduced physical resilience that can closely mimic low testosterone.
- Depression — shares fatigue, low motivation, reduced libido, and cognitive symptoms. The relationship between depression and testosterone is bidirectional — low testosterone may contribute to depression, and depression may suppress testosterone production.
- Perimenopause — the hormonal transition of perimenopause produces estrogen fluctuations that cause many of the same symptoms as low testosterone, and the two conditions frequently co-occur.
A comprehensive hormonal panel — including testosterone, estrogen, thyroid function, and relevant blood counts — is the appropriate starting point for evaluating unexplained fatigue, low libido, and mood changes in women.
What Causes Low Testosterone in Women
Several factors can reduce testosterone production or bioavailability in women:
Age and menopause — the most common cause. Testosterone production peaks in the early 20s and declines approximately 1% per year thereafter. By menopause, levels may be 50% of peak values. Women who undergo surgical menopause (ovary removal) experience a more abrupt and significant decline.
Hormonal contraception — combined oral contraceptives increase sex hormone-binding globulin (SHBG), which binds to testosterone and reduces the amount available to tissues. This is one mechanism through which the contraceptive pill can affect libido and energy in some women.
Hypopituitarism — conditions affecting the pituitary gland can reduce the hormonal signals that stimulate testosterone production in the ovaries and adrenal glands.
Adrenal insufficiency — the adrenal glands produce approximately 25% of women’s testosterone. Conditions affecting adrenal function can therefore reduce testosterone levels.
Chronic stress — sustained high cortisol levels, produced in response to chronic psychological or physical stress, can suppress testosterone production through the hormonal axis that governs sex hormone production.
Chronic illness — various conditions including autoimmune diseases, chronic kidney disease, and HIV can affect testosterone production.
Certain medications — including some antidepressants, opioid pain medications, and corticosteroids, can affect testosterone levels.
How to Increase Testosterone in Women: Evidence-Based Approaches

Lifestyle Interventions
Resistance training — the most consistently supported lifestyle intervention for supporting testosterone levels in women. Strength-based exercise involving compound movements (squats, deadlifts, rowing) has been shown to acutely increase testosterone levels and, with consistent practice over time, support the hormonal environment that maintains healthy levels. Aim for two to three sessions per week.
Optimize sleep — testosterone production occurs primarily during deep sleep. Chronic sleep deprivation — consistently fewer than seven hours per night — measurably reduces testosterone levels and compounds the fatigue and low mood that already characterize low testosterone. Addressing sleep quality is a foundational step, not an optional one.
Manage chronic stress — chronic elevated cortisol directly suppresses the hormonal signals that maintain testosterone production. This is one reason that women under sustained high stress frequently report reduced libido and energy: the hormonal consequence is real and measurable. Stress management approaches with a clinical evidence base include aerobic exercise, mindfulness-based practices, and professional psychological support.
Dietary considerations — adequate dietary fat intake supports sex hormone production, as testosterone is synthesized from cholesterol. Very low-fat diets can suppress testosterone production. Zinc — found in meat, shellfish, legumes, and seeds — is involved in testosterone synthesis and modest deficiency is associated with lower levels. Ensuring adequate protein intake supports muscle maintenance alongside hormonal health.
If you only have 10 minutes: Add one set of compound resistance exercises — squats, push-ups, or rows — to your day. The hormonal benefit of resistance training is dose-responsive: even a brief session produces an acute testosterone elevation and contributes to the longer-term hormonal environment that supports healthy levels.
Clinical Approaches
Testosterone therapy — off-label in many countries, testosterone therapy for women has a growing evidence base, particularly for postmenopausal women experiencing low libido that has not responded to estrogen therapy alone.
The International Society for the Study of Women’s Sexual Health (ISSWSH) and other clinical bodies have published guidelines supporting the use of low-dose testosterone therapy for women with hypoactive sexual desire disorder (HSDD) when other causes have been excluded. Available forms include compounded creams and gels applied topically, and — in some regions — approved patches.
Testosterone therapy for women uses doses significantly lower than those used in men, and is typically monitored with periodic blood tests to ensure levels remain within the physiological female range. Side effects at appropriate doses are generally mild.
Addressing underlying causes — if low testosterone is secondary to another condition (thyroid dysfunction, adrenal insufficiency, or medication effects), addressing the primary cause is typically the most effective approach.
If lifestyle approaches have not helped: Persistent symptoms — particularly reduced libido, significant fatigue, and low mood — that have not improved after consistent lifestyle modification over two to three months warrant a clinical evaluation including a hormonal blood panel. Self-directed interventions have real value, but their limits are also real. A physician or endocrinologist can identify which specific factor is driving the symptoms and recommend appropriate treatment.
Warning Signs: When to Seek Clinical Evaluation
The following warrant a clinical conversation rather than continued self-management:
- Significant fatigue that is not explained by sleep, stress, or identified medical conditions, and has persisted for more than four to six weeks
- A notable decline in sexual desire that is causing personal distress or affecting a close relationship
- Low mood, reduced motivation, or cognitive changes that are affecting daily functioning
- Irregular menstrual cycles without an obvious explanation
- Fertility concerns, particularly if ovulation appears irregular
- Symptoms that developed after starting hormonal contraception — worth discussing with the prescribing provider
- Symptoms following surgical menopause (ovary removal), where testosterone decline is particularly pronounced

Frequently Asked Questions
Can women have low testosterone? Yes. Testosterone is produced in women by the ovaries and adrenal glands and plays a direct role in libido, energy, muscle tone, mood, and bone health. Low testosterone is a recognized clinical condition in women, though it is significantly underdiagnosed because its symptoms are non-specific and often attributed to other causes.
What are the most common symptoms of low testosterone in women? The most commonly reported symptoms are reduced sexual desire, persistent fatigue and low energy, reduced muscle tone and strength, low mood and motivation, and in some cases cognitive fog. These symptoms overlap substantially with thyroid dysfunction, depression, and perimenopausal changes — which is why a blood test is the only reliable means of diagnosis.
How is low testosterone diagnosed in women? Through a blood test measuring total and free testosterone levels, ideally performed in the morning. Normal ranges for women are significantly lower than for men and vary by age. A comprehensive panel including thyroid function and other hormones is typically more informative than testosterone alone, given the overlap in symptoms between conditions.
Does the contraceptive pill affect testosterone in women? Yes, for some women. Combined oral contraceptives increase sex hormone-binding globulin (SHBG), which binds to testosterone and reduces its bioavailability. This is one mechanism through which hormonal contraception can affect libido and energy. If symptoms developed or worsened after starting a combined pill, discussing this with a prescribing provider is appropriate.
What is the normal testosterone level for women? Total testosterone in women typically falls between 15 and 70 ng/dL, though ranges vary by laboratory and age. Peak levels occur in the early 20s and decline gradually thereafter. Free testosterone — the biologically active fraction — is often the more clinically meaningful measurement. Interpretation should always be done in the context of symptoms, not numbers alone.
Is testosterone therapy safe for women? At doses appropriate for women — significantly lower than those used in men — testosterone therapy is generally considered safe when monitored appropriately. The International Society for the Study of Women’s Sexual Health supports its use for postmenopausal women with hypoactive sexual desire disorder when other causes have been excluded. It remains off-label in many countries. A physician specializing in women’s hormonal health can discuss whether it is appropriate for your situation.
The Bottom Line
Low testosterone in women is a real, diagnosable, and treatable condition that is systematically underrecognized — partly because testosterone has been framed as a male hormone, and partly because its symptoms overlap with so many other common conditions.
If you have been experiencing persistent fatigue, reduced sexual desire, low mood, and muscle weakness — and these symptoms have not been explained by thyroid function, iron levels, or other routine evaluations — asking your provider to include a testosterone measurement in your next blood panel is a reasonable and appropriate next step.
You deserve a complete evaluation. And the hormones that affect your energy, your desire, and your sense of vitality deserve to be part of that conversation.
References
- Cleveland Clinic. Low Testosterone in Women: Causes, Symptoms and Treatment. Updated April 2023. https://my.clevelandclinic.org/health/diseases/24897-low-testosterone-in-women
- Davis SR, et al. Global Consensus Position Statement on the Use of Testosterone Therapy for Women. Journal of Clinical Endocrinology & Metabolism. 2019;104(10):4660–4666.
- International Society for the Study of Women’s Sexual Health (ISSWSH). Testosterone Therapy in Women: Position Statement. 2021.
- Wierman ME, et al. Androgen therapy in women: a reappraisal. Journal of Clinical Endocrinology & Metabolism. 2014;99(10):3489–3510.
- National Institutes of Health, National Library of Medicine. Testosterone in Women. https://www.ncbi.nlm.nih.gov/books/NBK278940/
Related Articles on PureInti
- Low Libido in Women: Causes, Hormones, and Evidence-Based Solutions
- Perimenopause and Libido: Why Sex Drive Changes and What to Do
- Women’s Reproductive Health: A Complete Guide for Adults
- Vaginal Dryness: Causes, Natural Remedies, and When to Seek Treatment
- Weak Pelvic Floor Symptoms: Signs, Causes and Exercises