You noticed something unfamiliar. A bump, a sore, or an area of irritation in a place that made your stomach drop. Before you could think clearly, your mind had already arrived at the worst-case scenario — and then immediately doubled back, wondering whether it was actually just an ingrown hair, or friction, or nothing at all.
This experience — the sudden discovery, the private panic, the oscillation between catastrophizing and convincing yourself it is fine — is one of the most common and least talked-about moments in adult sexual health. And it deserves a better resource than a blurry image search at midnight.
This guide is written to provide exactly that: medically accurate, judgment-free information about herpes symptoms in women and men, how to distinguish herpes from other common skin conditions including ingrown hairs, how long you can have herpes without knowing, what testing and treatment involve, and what a positive result actually means for your health and your life.
Key Takeaways
- Herpes simplex virus (HSV) is one of the most common viral infections worldwide. The WHO estimates that approximately 67% of people under 50 have HSV-1, and approximately 11% have HSV-2 — meaning herpes is far more prevalent than most people realize.
- Most people with herpes have no noticeable symptoms or have symptoms so mild they go unrecognized. The majority of people who have herpes do not know it.
- Herpes vs ingrown hair is one of the most commonly searched comparisons — and for good reason. The two can appear similar on the skin. The key differences involve the character of the lesion, associated symptoms, and how it resolves over time.
- How long you can have herpes without knowing is indefinite — the virus can be present and transmissible without any outbreak occurring.
- Herpes is not curable, but it is highly manageable. Antiviral medication suppresses outbreaks, reduces viral shedding, and significantly lowers transmission risk. A herpes diagnosis does not define your sexual health or your future.
What Is Herpes and How Does It Spread
Herpes is caused by herpes simplex virus, which exists in two main types:
HSV-1 most commonly causes oral herpes — cold sores or fever blisters around the mouth — though it can also cause genital herpes through oral-to-genital contact. HSV-1 is extremely common, with WHO estimates suggesting approximately two-thirds of people under 50 carry the virus, often acquired in childhood through non-sexual contact.
HSV-2 most commonly causes genital herpes. It is transmitted primarily through genital-to-genital or oral-to-genital sexual contact. HSV-2 affects approximately 491 million people globally aged 15–49, according to the WHO.
Both types of herpes can infect the mouth, genitals, or other skin areas depending on the site of contact. Once acquired, the virus remains in the body permanently — residing in nerve cells and reactivating periodically to cause outbreaks, or remaining latent without producing any symptoms at all.
Herpes is transmitted through skin-to-skin contact with an infected area — including during periods when no visible sores are present, a phenomenon known as asymptomatic viral shedding. This is why herpes is so prevalent: it can be transmitted even when the infected person has no symptoms and is unaware they carry the virus.
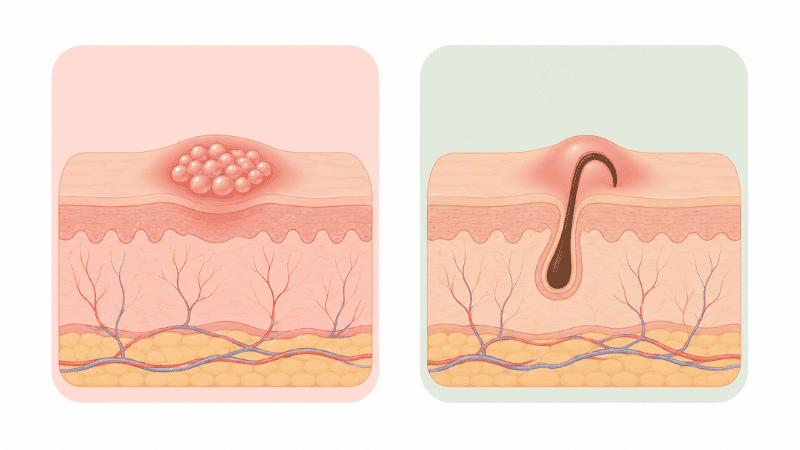
Herpes vs Ingrown Hair: How to Tell the Difference
This is the question that brings many people to this page, and it deserves a direct, clinically grounded answer.
Both herpes sores and ingrown hairs can appear as small bumps or sores in the genital area. Both can cause discomfort or tenderness. From a visual inspection alone — particularly without clinical training — they can be genuinely difficult to distinguish. This is why a clinical evaluation is the only reliable means of diagnosis: not because you cannot observe the difference, but because the consequences of a misidentification in either direction are significant.
Characteristics of Herpes Sores
Herpes outbreaks typically present as:
- Small fluid-filled blisters (vesicles) that appear in clusters, often on the genitals, buttocks, inner thighs, or around the anus
- Blisters that rupture within one to four days, leaving shallow, painful ulcers that crust over and heal — typically within two to four weeks during a first outbreak, and more quickly in subsequent outbreaks
- Associated symptoms during a first outbreak often include flu-like symptoms — fever, swollen lymph nodes, muscle aches — that do not accompany ingrown hairs
- Tingling, burning, or itching in the affected area before blisters appear (a prodromal period) — a characteristic feature of herpes that helps distinguish it from other skin conditions
- Pain that is often described as burning or stinging rather than the localized ache of an ingrown hair
Characteristics of Ingrown Hairs
Ingrown hairs occur when a hair grows back into the skin rather than outward, typically after shaving, waxing, or other hair removal. They present as:
- A single raised bump, often with a visible hair beneath the skin surface
- Flesh-colored or red appearance, sometimes with a yellow or white center if pus has accumulated (indicating a mild infection)
- Tenderness that is localized to the specific bump rather than diffuse over a broader area
- No associated systemic symptoms — no fever, no swollen lymph nodes, no tingling prodrome
- Resolution typically within one to two weeks without specific treatment, often improving on its own as the hair grows out
The Key Distinguishing Features
| Feature | Herpes | Ingrown Hair |
|---|---|---|
| Appearance | Clusters of small blisters | Single bump, often with visible hair |
| Progression | Blisters → ulcers → crust → heal | Bump gradually resolves or may become pus-filled |
| Associated symptoms | Tingling prodrome, possible fever and flu symptoms | None |
| Location pattern | Often in clusters, may recur in same area | Single lesion, common in shaved areas |
| Pain character | Burning, stinging, diffuse | Localized tenderness |
| Resolution | 2–4 weeks (first outbreak), faster subsequently | 1–2 weeks without treatment |
The bottom line on herpes vs ingrown hair: If you are genuinely unsure which you are looking at — and particularly if there are multiple lesions, systemic symptoms, or the area is in a location that could indicate herpes — a clinical evaluation and swab test during an active outbreak is the definitive means of diagnosis. Do not attempt to self-diagnose based on visual inspection alone.
How Long Can You Have Herpes Without Knowing
The answer to this question is one of the most important and least understood aspects of herpes: indefinitely.
Herpes can be present in your body without ever producing a noticeable outbreak. The majority of people with herpes — estimates vary, but research suggests 80–90% of those with HSV-2 — are either completely unaware of their infection or attribute mild, atypical symptoms to other causes.
Symptoms that are often misattributed rather than recognized as herpes include:
- Mild genital discomfort or itching attributed to friction or laundry detergent
- Small cuts or fissures attributed to dryness or vigorous activity
- A brief episode of discomfort that resolved without medical attention
The window period for herpes blood antibody testing — the time from infection to reliable detection — is typically 12–16 weeks. Testing too early may return a false negative not because of test inaccuracy but because antibodies have not yet developed to detectable levels.
This means you can carry and transmit herpes for months or years without knowing. This is not a failure of attentiveness — it is a characteristic of the virus itself. The implication is that a herpes diagnosis in a current relationship does not necessarily indicate recent transmission or infidelity: the infection may have been present for years in either partner.
Herpes Symptoms in Women: What to Expect
Herpes symptoms in women are frequently absent or atypical. When a first outbreak does occur, it typically appears within two to twelve days of initial exposure and is often the most severe outbreak a person will experience. Subsequent outbreaks are generally shorter, milder, and less frequent over time.
First outbreak symptoms in women may include:
- Blisters or sores on the vulva, vagina, cervix, buttocks, or inner thighs
- Burning, itching, or tingling in the affected area before blisters appear
- Pain during urination if sores are near the urethra
- Vaginal discharge that may be unusual in character
- Flu-like symptoms including fever, body aches, and swollen lymph nodes — more common in first outbreaks than recurrences
Recurrent outbreaks are typically shorter (three to seven days), less painful, and may be preceded by a tingling or burning prodrome in the same location. Common triggers for recurrence include stress, illness, hormonal changes including the menstrual cycle, and immune suppression.
Many women with herpes have infrequent outbreaks or none at all after the initial infection. The virus does not go away, but for many people it becomes essentially inactive over time.
Herpes Symptoms in Men: What to Expect
Herpes symptoms in men follow a similar pattern but present in different anatomical locations. Men are somewhat more likely than women to experience noticeable symptoms, though many still have mild or unrecognized outbreaks.
First outbreak symptoms in men may include:
- Blisters or sores on the penis, scrotum, buttocks, inner thighs, or around the anus
- Burning or tingling before blisters appear
- Pain or discomfort during urination if sores are near the urethra
- Swollen lymph nodes in the groin
- Flu-like symptoms during a first outbreak
Recurrent outbreaks in men are generally milder and shorter than the initial outbreak, and typically recur in the same anatomical area. Some men experience a clear prodrome — tingling or numbness — that reliably predicts an impending outbreak, which can guide decisions about antiviral medication and sexual activity.
What Happens If Herpes Is Left Untreated
Unlike bacterial STIs such as chlamydia and gonorrhea, herpes does not cause the same type of progressive tissue damage when left untreated. The virus remains latent in nerve cells and does not invade other organ systems in people with healthy immune function.
However, leaving herpes unmanaged has several meaningful consequences:
Transmission risk remains elevated. Without antiviral medication, viral shedding occurs more frequently, increasing the likelihood of transmitting the virus to sexual partners — including during periods with no visible symptoms.
Outbreaks may be more frequent and severe. Antiviral medication significantly reduces outbreak frequency and severity. Without treatment, some people experience frequent recurrences that substantially affect quality of life.
Neonatal herpes risk. For pregnant women with herpes — particularly those who acquire a new herpes infection in the third trimester — the risk of transmitting the virus to the newborn during delivery is a serious concern. This is why herpes status is discussed during prenatal care, and why antiviral suppressive therapy is recommended for pregnant women with herpes.
Complications in immunocompromised individuals. People with significantly weakened immune systems — including those with HIV — may experience more severe, persistent, or widespread herpes outbreaks that warrant aggressive antiviral management.
Herpes Testing: What to Expect
Two types of herpes tests are commonly used, and understanding the difference is important for interpreting results accurately.
Viral swab test (PCR or culture): The most accurate test for diagnosing an active outbreak. A swab is taken directly from an active sore or blister. This test is most accurate when performed within the first 24–48 hours of a lesion appearing. A negative swab does not rule out herpes if no active lesion is present.
Blood antibody test (IgG): Detects antibodies to HSV-1 or HSV-2 in the bloodstream, indicating previous infection regardless of whether an outbreak is currently present. This test is most accurate 12–16 weeks after potential exposure. It can identify which type of herpes (HSV-1 or HSV-2) is present. However, it can produce false positives — particularly at low positive values — and false negatives if performed too soon after exposure.
Routine STI panels do not always include herpes blood testing. If you want to be tested for herpes specifically, request it explicitly and discuss with your provider whether a swab test, blood test, or both are appropriate for your situation.
If you only have 10 minutes: If you have an active sore right now that you are concerned about, contact a sexual health clinic or your primary care provider today to arrange a swab test. The window for the most accurate swab result is short — within the first 24–48 hours of a lesion appearing. Do not wait.
Herpes Treatment: What Is Available
While there is no cure for herpes, highly effective antiviral medications are available that transform the experience of living with the virus for most people.
Episodic antiviral therapy — taken at the first sign of an outbreak or prodrome — shortens the duration and severity of individual outbreaks. Aciclovir, valaciclovir (valacyclovir), and famciclovir are the most commonly used antivirals. All are taken orally and are generally well-tolerated.
Suppressive antiviral therapy — taken daily regardless of whether an outbreak is occurring — reduces outbreak frequency, often dramatically, and significantly lowers the risk of transmitting the virus to a sexual partner. Research has shown that daily suppressive therapy with valaciclovir reduces the risk of HSV-2 transmission by approximately 50% in serodiscordant couples (where one partner has herpes and the other does not), in combination with consistent condom use.
For many people with herpes, suppressive therapy is the preferred approach because it removes the need to identify and respond to outbreaks individually, provides ongoing protection for partners, and significantly reduces the psychological burden of the infection.
The decision between episodic and suppressive therapy depends on the frequency of outbreaks, the presence of a partner without herpes, and individual preference — a conversation to have with a healthcare provider.
Warning Signs: When to Seek Prompt Medical Attention
- An active genital sore or blister that you believe may be herpes — seek a swab test within 24–48 hours for the most accurate result
- Severe pain during a first outbreak, particularly if it prevents urination
- Herpes symptoms in a newborn following birth to a mother with herpes — seek immediate pediatric evaluation
- Signs of herpes encephalitis — severe headache, confusion, fever, or neck stiffness — which is a rare but serious complication requiring urgent medical care
- Any concern about herpes exposure during pregnancy — discuss with your obstetric provider promptly
- Frequent or severe outbreaks that are significantly affecting quality of life — suppressive therapy can help
Frequently Asked Questions
How do you tell the difference between herpes and an ingrown hair? The key distinguishing features are the character and progression of the lesion. Herpes typically presents as clusters of small fluid-filled blisters that rupture and ulcerate, often with a tingling prodrome and sometimes flu-like symptoms. Ingrown hairs typically appear as single bumps with a visible hair beneath the skin, resolve within one to two weeks, and produce no systemic symptoms. Visual inspection alone is unreliable — a clinical evaluation and swab test during an active outbreak is the definitive means of diagnosis.
How long can you have herpes without knowing? Indefinitely. The majority of people with herpes have no recognizable symptoms or have symptoms so mild they are attributed to other causes. The virus can be present and transmissible for months or years without producing a noticeable outbreak. A blood antibody test performed 12–16 weeks after potential exposure is the most reliable means of detection in the absence of active symptoms.
Can you have herpes without any symptoms? Yes — and this is the norm rather than the exception. An estimated 80–90% of people with HSV-2 are unaware of their infection. Asymptomatic viral shedding — during which the virus is transmissible even without visible sores — occurs regularly in people who have never had a recognized outbreak.
What are the first signs of herpes? In a first outbreak, herpes often begins with a tingling, burning, or itching sensation in the affected area before blisters appear. This prodromal period typically lasts one to two days. Flu-like symptoms — fever, muscle aches, swollen lymph nodes — are common during a first outbreak. The blisters themselves then appear, typically in clusters, rupture within a few days, and heal over one to four weeks.
Is herpes curable? No — the herpes simplex virus remains in the body permanently once acquired, residing in nerve cells. However, it is highly manageable. Antiviral medication reduces outbreak frequency and severity, lowers transmission risk, and for many people with suppressive therapy, outbreaks become rare or absent. A herpes diagnosis is a manageable chronic condition, not a health crisis.
Does herpes go away on its own? Individual outbreaks resolve on their own within one to four weeks for a first outbreak, and more quickly for recurrences. The virus itself does not leave the body. Without antiviral treatment, outbreaks will continue to occur — though for many people they become less frequent over time as the immune system develops a stronger response to the virus.
How is herpes transmitted? Herpes is transmitted through skin-to-skin contact with an infected area — including during periods with no visible sores, a phenomenon known as asymptomatic viral shedding. It can be transmitted through vaginal, anal, and oral sexual contact, and — in the case of HSV-1 — through kissing or other non-sexual skin contact. Condoms significantly reduce but do not eliminate transmission risk, as herpes can be present on skin not covered by a condom.
The Bottom Line
A herpes diagnosis — or the concern that you may have herpes — is one of the most emotionally charged moments in sexual health. The stigma associated with the virus is significantly disproportionate to its actual medical impact, which for most people with access to antiviral medication is minimal.
Herpes is common, manageable, and — with the right information and medical support — liveable with in every meaningful sense. The most important steps are getting accurately tested, understanding your treatment options, and having the conversations with partners and healthcare providers that allow you to make informed decisions.
If this guide has raised questions about your own situation, a sexual health clinic or primary care provider can provide the clinical evaluation, accurate testing, and honest support you deserve.
References
- World Health Organization. Herpes Simplex Virus. Updated April 2023. https://www.who.int/news-room/fact-sheets/detail/herpes-simplex-virus
- Centers for Disease Control and Prevention. Genital Herpes — CDC Detailed Fact Sheet. Updated April 2024. https://www.cdc.gov/std/herpes/stdfact-herpes-detailed.htm
- Corey L, et al. Once-daily valacyclovir to reduce the risk of transmission of genital herpes. New England Journal of Medicine. 2004;350(1):11–20.
- Johnston C, Corey L. Current Concepts for Genital Herpes Simplex Virus Infection. Clinical Infectious Diseases. 2016;62(Suppl 4):S249–S255.
- National Institutes of Health, National Library of Medicine. Herpes Simplex. https://www.ncbi.nlm.nih.gov/books/NBK554427/