Pain during sex is one of those experiences that many people endure quietly for far longer than they should. It might start gradually — a discomfort that you attribute to stress, or position, or not being relaxed enough. You adjust. You accommodate. You say nothing, because how do you begin that conversation, and with whom?
Weeks become months. The discomfort becomes expected. And somewhere in the process, the idea that this might be a medical concern — one with identifiable causes and effective treatment — stops feeling like a realistic possibility.
It is. Pain during sex, clinically termed dyspareunia, affects an estimated three in four women at some point in their lives according to the American College of Obstetricians and Gynecologists. It also affects men, though it is less frequently discussed in that context. In the vast majority of cases, it has a diagnosable cause and responds to appropriate treatment.
This guide covers what causes pain during sex, how those causes differ by life stage and context, what treatment options exist, and how to approach the clinical conversation you may have been putting off.
Key Takeaways
- Pain during sex (dyspareunia) affects approximately three in four women at some point, and is significantly underreported — many people manage it privately for years without seeking care.
- Pain can be superficial (at the entrance) or deep (during deeper penetration), and the location is an important diagnostic clue that points toward different underlying causes.
- The most common causes include vaginal dryness from hormonal changes, vaginismus (involuntary pelvic floor muscle tension), endometriosis, pelvic inflammatory disease, and skin conditions affecting the vulva.
- Psychological factors — including anxiety, past trauma, and performance pressure — can cause or significantly worsen physical pain during sex through a well-documented neurological mechanism.
- Pain during sex is not a normal baseline to accept at any age. Effective treatment is available for the majority of causes, and early intervention consistently produces better outcomes than prolonged accommodation.
Why Is Sex Painful? Understanding the Mechanism
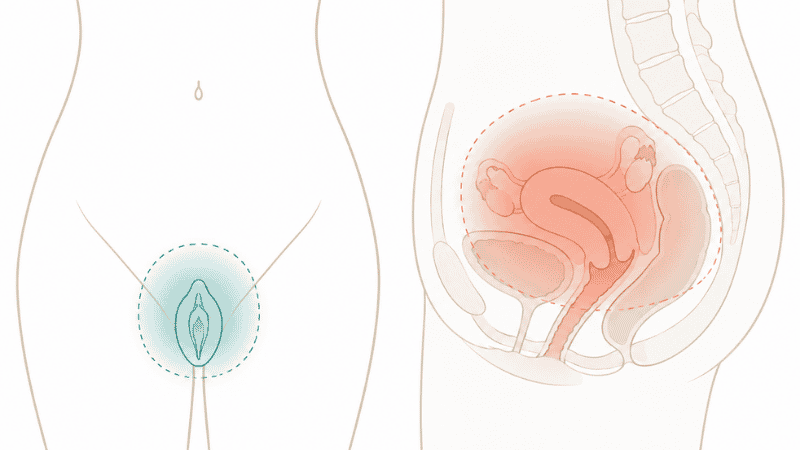
Pain during sex is not a single condition — it is a symptom with multiple possible origins. The location, timing, and character of the pain provide important diagnostic information that helps direct appropriate investigation and treatment.
Superficial or entry pain — felt at the vaginal opening at the beginning of penetration — most commonly points to vaginal dryness, skin conditions of the vulva, vaginismus, or vulvodynia (chronic vulvar pain without an identifiable cause).
Deep pain — felt internally during deeper penetration — is more commonly associated with endometriosis, pelvic inflammatory disease, uterine fibroids, ovarian cysts, or pelvic floor dysfunction affecting the deeper muscle layers.
Pain occurring only in certain positions typically points to a specific anatomical or musculoskeletal cause — such as a retroverted uterus, pelvic floor tension, or a cyst that is being compressed in particular positions.
Pain after sex that lingers for hours is often associated with endometriosis, pelvic congestion syndrome, or uterine conditions, and deserves specific clinical attention.
Understanding which category applies to your experience is the most useful information you can bring to a clinical appointment.
Common Causes of Pain During Sex in Women
Vaginal Dryness and Estrogen Decline
Insufficient vaginal lubrication is the most common cause of superficial pain during sex in women across all age groups. It can result from reduced arousal time, hormonal contraception, breastfeeding, antidepressant use, or the estrogen decline of perimenopause and menopause.
When estrogen levels fall — whether temporarily or as part of menopause — vaginal tissue thins, loses elasticity, and produces less natural lubrication. The resulting friction causes pain that ranges from mild discomfort to significant sharp pain. Over time, this can create a cycle: anticipated pain leads to reduced arousal, which reduces lubrication, which worsens pain.
Vaginal moisturizers used regularly and lubricants used during sexual activity are effective first-line approaches for mild to moderate dryness. For postmenopausal women, low-dose vaginal estrogen addresses the underlying hormonal cause rather than just the symptom, and is considered safe and highly effective for long-term use by most women.
Vaginismus
Vaginismus is an involuntary contraction of the pelvic floor muscles surrounding the vaginal entrance, making penetration painful or impossible. It is not a conscious choice — the muscle response occurs automatically, often triggered by anticipation of pain, anxiety, or a conditioned response from a previous painful experience.
Vaginismus can be lifelong (primary) — present from the first attempt at penetration — or secondary, developing after a period of pain-free sexual activity. It is one of the most treatable causes of painful sex, with pelvic floor physical therapy producing high success rates through a gradual desensitization process that allows the muscles to learn a different response.
Vulvodynia
Vulvodynia is chronic vulvar pain — burning, stinging, or rawness — that occurs without an identifiable infection or dermatological cause. It may be localized to the vaginal opening (vestibulodynia) or generalized across the vulva. It can be provoked by touch or pressure, or unprovoked and constant.
The cause of vulvodynia is not fully understood, but current research points to sensitization of the peripheral nerves of the vulvar tissue — a process in which the nervous system becomes hyperresponsive to stimuli that would not normally cause pain. Treatment approaches include topical medications, pelvic floor physical therapy, cognitive behavioral therapy, and in some cases nerve-targeted medications.
Painful Sex After Menopause
Painful sex after menopause is among the most common — and most consistently untreated — sexual health concerns in women over 50. The condition is formally termed genitourinary syndrome of menopause (GSM), and it encompasses vaginal dryness, tissue thinning, reduced elasticity, and increased vulnerability to friction and irritation.
Unlike hot flashes, which typically improve over time without treatment, GSM does not self-resolve — it tends to worsen progressively without intervention. This is clinically important because many women assume postmenopausal pain during sex is an inevitable consequence of aging that cannot be addressed. It is not. Low-dose vaginal estrogen, vaginal hyaluronic acid moisturizers, and ospemifene (an oral non-hormonal option) are all effective, evidence-based treatments.
If you have been experiencing pain during sex since menopause and have not raised it with your provider, this conversation is worth having. The treatment options are straightforward and the improvement in quality of life is significant.
Pelvic Pain During Sex: Endometriosis
Endometriosis is a condition in which tissue similar to the uterine lining grows outside the uterus — on the ovaries, fallopian tubes, bladder, bowel, or pelvic ligaments. Deep pain during sex is one of the most characteristic symptoms, often described as a sharp, stabbing, or aching sensation felt internally, particularly in positions involving deeper penetration.
Endometriosis affects an estimated one in ten women of reproductive age, yet the average time from symptom onset to diagnosis is seven to ten years. Painful sex is a key symptom that, when present alongside painful periods and pelvic pain at other times, should prompt evaluation for endometriosis rather than symptom management alone.
Treatment ranges from hormonal management to laparoscopic surgical removal of endometrial lesions, and is tailored to symptom severity and reproductive plans.
Pelvic Inflammatory Disease and Infections
Pelvic inflammatory disease (PID) — an infection of the uterus, fallopian tubes, or ovaries, most commonly caused by untreated chlamydia or gonorrhea — produces deep pelvic pain during sex alongside other symptoms including abnormal discharge, fever, and pelvic tenderness. PID requires prompt antibiotic treatment and, if suspected, urgent clinical evaluation.
Other infections including yeast infections, bacterial vaginosis, and herpes can cause vulvar inflammation and pain during sex that typically resolves with appropriate treatment of the underlying infection.
Painful Sex After Pregnancy
Painful sex after pregnancy is extremely common and significantly underacknowledged. The combination of hormonal changes (particularly the estrogen suppression of breastfeeding), physical recovery from vaginal delivery, perineal trauma, and psychological adjustment to postpartum life creates conditions in which pain during sex is nearly universal in the early postpartum months.
For most women, this improves gradually over three to six months. Vaginal dryness is particularly prominent in breastfeeding women — a direct consequence of the hormonal suppression of estrogen during lactation — and responds well to lubricants and vaginal moisturizers. Pelvic floor physical therapy is particularly valuable for women who experienced perineal tears or significant pelvic floor strain during delivery.
If pain during sex persists beyond six months postpartum or is severe enough to prevent resuming sexual activity, a gynecological evaluation is appropriate.
Pain During Sex in Men: An Underrecognized Concern
Pain during sex is less commonly discussed in men but is not rare. It can manifest as pain at the tip or shaft of the penis, in the testicles, or as deep pelvic pain.
Common causes include phimosis (tight foreskin), skin conditions affecting the penis, prostatitis (inflammation of the prostate), pelvic floor dysfunction, and infections including STIs. Pelvic floor tension in men — analogous to vaginismus in women — is an underrecognized cause of pain during sex and responds to targeted pelvic floor physical therapy.
Men experiencing consistent pain during sex deserve the same clinical attention as women, and the same encouragement to raise the concern with a healthcare provider.
The Psychological Dimension of Painful Sex
Pain during sex does not occur in isolation from psychological experience — and the relationship runs in both directions.
Anxiety, anticipation of pain, past difficult experiences, and negative beliefs about sex or one’s own body can all produce or amplify physical pain through well-documented neurological pathways. Chronic pain causes the nervous system to become sensitized — meaning that over time, stimuli that would not normally trigger pain begin to do so, because the system has been conditioned toward a pain response.
This does not mean the pain is imaginary or primarily psychological in origin. It means that in many cases, addressing both the physical and psychological dimensions of painful sex produces better outcomes than treating either in isolation. Cognitive behavioral therapy (CBT) adapted for sexual pain, mindfulness-based approaches, and sex therapy have all demonstrated effectiveness alongside physical treatment.
For couples, the impact of painful sex on intimacy and relationship dynamics is real and significant. Open communication — discussed in detail in our relationship communication guide — and, where needed, couples therapy can support both partners through the process of addressing and resolving painful sex.
Evidence-Based Treatment Approaches
First-Line Self-Management
For mild to moderate pain primarily related to dryness or insufficient arousal:
- Allow adequate time for arousal before penetration — natural lubrication increases significantly with extended arousal time
- Use a high-quality water-based or silicone-based lubricant consistently
- Apply a vaginal moisturizer (particularly hyaluronic acid-based) two to three times per week for ongoing tissue health
- Avoid products that can irritate vulvar tissue — fragranced soaps, bubble baths, scented pads, and douches
If you only have 10 minutes: Apply a vaginal moisturizer before bed tonight. Used consistently two to three times per week, this single step produces measurable tissue improvement within four to six weeks and is the most accessible starting point for dryness-related pain.
Pelvic Floor Physical Therapy
For vaginismus, pelvic floor tension, postpartum pelvic floor trauma, and deep pelvic pain — pelvic floor physical therapy is the gold standard evidence-based intervention. Treatment involves internal and external assessment of muscle tone and coordination, manual therapy, graduated desensitization exercises, and biofeedback.
Most people with vaginismus achieve significant improvement within eight to sixteen weeks of specialist treatment. This is a condition that responds reliably to appropriate physical therapy — not something to accept as permanent.
Clinical and Medical Treatment
Depending on the identified cause, clinical options may include low-dose vaginal estrogen for GSM, hormonal management for endometriosis, antibiotic treatment for infections, topical lidocaine for vulvodynia, or surgical intervention for structural causes.
If self-directed approaches have not helped after six to eight weeks: This is the signal to make a clinical appointment rather than continuing to self-manage. Persistent pain during sex has identifiable causes in the majority of cases, and a gynecologist, sexual health specialist, or pelvic floor physiotherapist can direct appropriate investigation and treatment.
Warning Signs: When to Seek Urgent or Prompt Medical Attention
The following warrant clinical evaluation without delay:
- Pain during sex accompanied by fever, abnormal discharge with odor, or significant pelvic tenderness — possible signs of pelvic inflammatory disease requiring prompt treatment
- New or worsening deep pelvic pain during sex, particularly with painful periods — warrants evaluation for endometriosis or other pelvic conditions
- Pain during sex following a procedure, IUD insertion, or pelvic surgery
- Postmenopausal bleeding — any vaginal bleeding after menopause requires prompt evaluation
- Pain during sex that is severe, sudden in onset, or accompanied by other new symptoms
- Any concern about possible STI exposure alongside pain
These are clinical circumstances requiring a medical appointment — not situations for continued self-management.

Frequently Asked Questions
Why does sex hurt even when I am aroused? Arousal is one factor in vaginal lubrication, but not the only one. Hormonal factors — including estrogen levels affected by contraception, breastfeeding, or menopause — can significantly reduce lubrication independent of arousal. Conditions including vaginismus, vulvodynia, and skin conditions of the vulva can also cause pain that occurs despite adequate arousal. A clinical evaluation can identify which factor is primary.
Is pain during sex normal? Occasional mild discomfort due to a specific situational cause — inadequate lubrication, certain positions, hormonal fluctuation — can occur. Persistent, recurring, or significant pain during sex is not a normal baseline to accept. It has identifiable causes and, in the majority of cases, effective treatments. Normalizing it is one of the primary reasons it goes untreated for years.
What causes painful sex after menopause? The primary cause is the estrogen decline of menopause, which causes vaginal tissue to thin, lose elasticity, and produce less natural lubrication — a condition called genitourinary syndrome of menopause (GSM). Unlike menopausal hot flashes, GSM does not improve over time without treatment. Low-dose vaginal estrogen, vaginal moisturizers, and other evidence-based options are effective and should be discussed with your provider.
Can anxiety cause pain during sex? Yes. Anxiety and anticipation of pain activate the nervous system in ways that increase muscle tension, reduce arousal response, and lower pain thresholds — all of which can directly contribute to pain during sex. Vaginismus, for example, is largely driven by an involuntary anxiety-based muscle response. Addressing the psychological dimension alongside any physical causes consistently produces better outcomes than treating either in isolation.
How long is painful sex after pregnancy normal? Some discomfort in the first six to eight weeks postpartum is expected, particularly following vaginal delivery. Significant pain beyond three months postpartum — especially in women who are breastfeeding — often reflects vaginal dryness from hormonal suppression of estrogen, which responds well to lubricants and vaginal moisturizers. Pain persisting beyond six months, or pain severe enough to prevent resuming sexual activity, warrants a gynecological evaluation.
When should I see a doctor about pain during sex? If pain during sex is recurring, worsening, or has been present for more than a few weeks without an obvious situational explanation, a clinical evaluation is appropriate. Additional reasons to seek prompt care: pain accompanied by fever or unusual discharge, deep pelvic pain with painful periods, postmenopausal bleeding, or pain that has not responded to lubricants and moisturizers after six to eight weeks of consistent use.
Can pain during sex be cured? In most cases, yes — or significantly improved. The outcome depends on the underlying cause. Vaginismus has high resolution rates with pelvic floor physical therapy. GSM responds reliably to vaginal estrogen. Infections resolve with treatment. Endometriosis can be managed hormonally or surgically. Even complex conditions including vulvodynia, for which no single cure exists, respond to multimodal treatment approaches that significantly reduce pain and improve quality of life.
The Bottom Line
Pain during sex is common, has identifiable causes, and responds to treatment. The most significant barrier to resolution is not the absence of effective options — it is the deeply ingrained tendency to accept it, accommodate it, and say nothing.
The conversation with a healthcare provider is easier than you expect. It happens in clinical practice every day. And addressing the cause of pain during sex — rather than managing around it — restores something that has real significance for your quality of life, your relationships, and your overall well-being.
You deserve to be comfortable. That is not a small thing.
References
- American College of Obstetricians and Gynecologists. When Sex Is Painful. Updated 2023. https://www.acog.org/womens-health/faqs/when-sex-is-painful
- Cleveland Clinic. Dyspareunia (Painful Intercourse): Causes and Treatment. Updated July 2024. https://my.clevelandclinic.org/health/diseases/12325-dyspareunia-painful-intercourse
- Bornstein J, et al. 2015 ISSVD, ISSWSH and IPPS Consensus Terminology and Classification of Persistent Vulvar Pain and Vulvodynia. Obstetrics & Gynecology. 2016;127(4):745–751.
- The Menopause Society. Genitourinary Syndrome of Menopause. https://menopause.org/patient-education/menopause-topics/sexual-health
- National Institutes of Health, National Library of Medicine. Dyspareunia. https://www.ncbi.nlm.nih.gov/books/NBK562247/
Related Articles on PureInti
- Vaginal Dryness: Causes, Natural Remedies, and When to Seek Treatment
- Weak Pelvic Floor Symptoms: Signs, Causes and Exercises
- Low Libido in Women: Causes, Hormones, and Evidence-Based Solutions
- Women’s Reproductive Health: A Complete Guide for Adults
- How to Communicate in a Relationship: A Practical Guide